
Rediscover the Art of Listening with Srava.
Unify Unstructured Clinical Data and Fuel Actionable Intelligence.
Stop managing documents. Start orchestrating intelligence.
The risk profile of your patient does not change from setting to setting.
Risk Adjustment is all about HCCs.

Limitless Diagnostic Power.
Simplify Clinical Documentation, Clinical Data and Leverage AI.

One source to generate, ingest, store and process your data. Share data across EHRs with intelligent automation. Create an intelligent healthcare system.

We currently serve
We generate
We process

Bring Clinical Documents to life
From audio capture, automatic speech recognition, ambient listening to centralized storage and retrieval Saince platform can bring you clinical documentation to life.

Connect across EHRs
Create automated workflows to store and share clinical documentation across your health system.

Ensure business continuity
With healthcare systems under constant attack by cyber criminals, you need a system that stays insulated.
Srava is not a novel tech idea by a silicon valley startup trying to learn clinical documentation. Srava is a solution synthesized by bringing together 24 years of clinical documentation experience. We documented several million patient health journeys and leveraged all that knowledge and experience to create a solution that helps you reduce your physician’s cognitive burden so that they can connect better and practice better medicine.

Explore our products.
The First Ambient AI Scribe Designed Exclusively for Psychiatric Health. Available to You Now on Doc-U-Scribe.
- No specific dictation commands required
- Captures multi-speaker dialogue naturally
- Allows for uninterrupted patient narratives
Unify unstructured clinical data and fuel actionable intelligence.
- Medical Document Ingestion & Automation
- EHR Legacy Data Archiving & Content Repository
- Automated Clinical Workflow & Routing
- Interoperability Gateway for EHR Integration

The risk profile of your patient does not change from setting to setting.
- Boost CDIS productivity
- Improve efficiency with integrated encoder
- Machine-learning enabled NLP
- HAC, PSI and QA Measure identification
- Guaranteed ROI in 3 months or less

Doc-U-Aide makes HCC identification, tracking and documentation easy.
- Customized Workflows
- Coding Precision
- Documentation Enhancement
- Education and Training
- Continuous Oversight

World-class diagnostic clarity. Streamlined for speed. The PACS you need for a high-velocity workflow.
- Zero Distractions
- Maximum Uptime
- Global Standard
See deeper. Diagnose faster. The most advanced AI-powered imaging platform we have ever built.
- Conversational AI Reporting
- Auto-Impression Generation
- Intelligent Staging
- Burnout Reduction

Engineered for the Future. Built for You.
- Patient Registration & Appointment Scheduling
- Comprehensive EHR & Medical Records
- Revenue Cycle & Insurance Management
- Integrated Clinical Services (Labs, Radiology, Pharmacy)
- Inventory & Supply Chain Mastery
- Global Compliance. Local Trust.


Master the business of radiology.
- Intelligent Scheduling & Patient Tracking
- Automated DICOM Modality Worklist (DMWL)
- Integrated Reporting & Dictation
- Scanalytics & Business Intelligence
- Streamlined Billing & Inventory

Trusted by clients globally.


















What our customers say.
Srava has completely transformed my sessions. I no longer break eye contact to jot down notes. Patients feel heard, and I feel more present. The structured draft waiting at the end is a game-changer.

I used to spend hours after clinic finishing notes. With Srava, my ‘pajama time’ is gone. It organizes patient narratives into SOAP notes and MSE drafts automatically, saving me precious time.

The Enterprise version is a revelation. For the first time, we can view a patient’s risk profile across inpatient and outpatient settings in one place. This continuity has improved both documentation integrity and patient safety reviews.
Saince PACS is a very good platform for radiology reporting. It gives easy access and provides a very good viewer for reporting. The 3D viewer is very convenient for imaging.
I have been using Saince PACS for the last two years and had really very good experience. Very less downtime and whenever it goes down the response from the team was very prompt. It has all the features you desire in your PACS such as MPR and DICOM export etc. Easy to handle.
Saince PACS came with many updates and upgrades recently. Great work from the team.
Latest news from Saince.

Your Telehealth Recordings Are a Compliance Time Bomb. Here's How to Defuse It.
If your health system has an active telehealth program, someone in your organization is sitting on a compliance problem they probably don't know about yet. It will surface — through a HIPAA audit, ...
Read More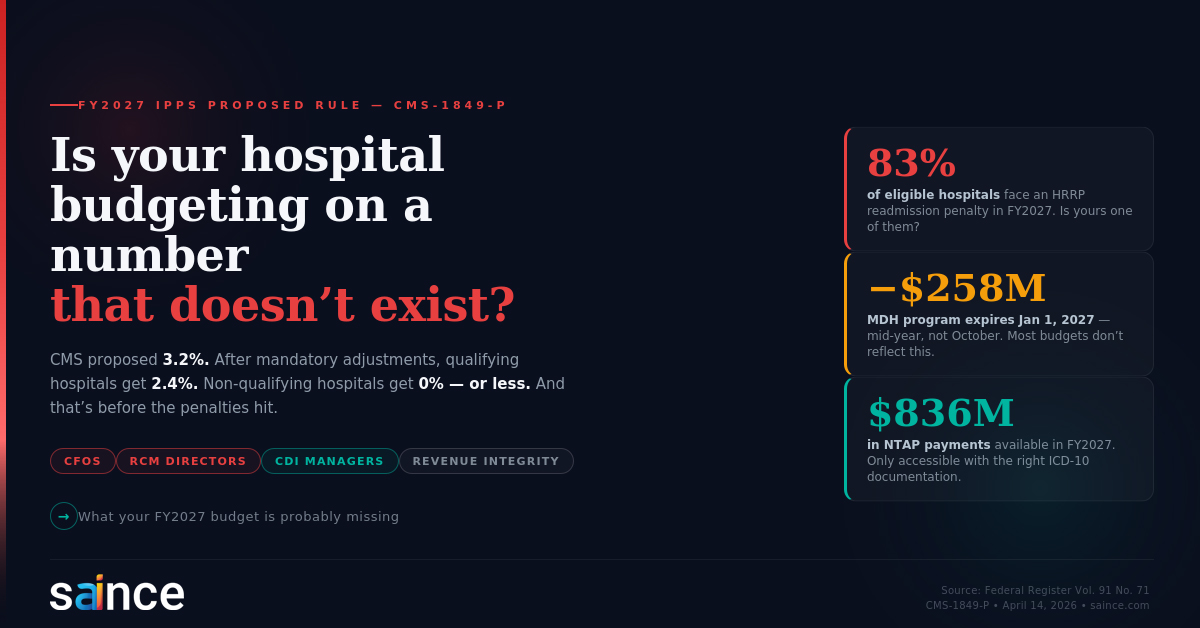
Is your hospital budgeting on a number that doesn't exist?
The FY2027 IPPS Proposed Rule: What the Payment Numbers Don't Tell You — and Why CDI Has Never Mattered More On April 14, 2026, CMS published the FY2027 Inpatient Prospective Payment System ...
Read More
The 8 Clinical Content Types Your EHR Cannot Handle — And What to Do About Each One
Every HIM Director knows the feeling. You open the queue on Monday morning, and before you can touch the structured work — the coding queries, the CDI reviews, the compliance reports — you have t...
Read More